Overview & Epidemiology
Periprosthetic fractures — fractures occurring around an orthopaedic implant — are one of the most challenging complications in arthroplasty surgery, requiring combined trauma and arthroplasty expertise. Their incidence is rising as the number of primary and revision arthroplasties increases and the population ages. Periprosthetic fractures around the hip (femoral or acetabular) are the most common, followed by the knee, then shoulder. They carry significant morbidity: 15–20% one-year mortality in frail elderly patients, high re-operation rates, and prolonged rehabilitation. Management depends on fracture location, implant stability, bone stock quality, and patient factors.
- Incidence: postoperative periprosthetic femoral fractures occur in 0.4–3.5% after primary THA and up to 4% after revision THA; intraoperative fractures are more common during uncemented THA (5.4%) than cemented THA (0.3%), and during revision surgery (20.9%); periprosthetic femoral fractures are the third most common reason for revision after THA overall, and the second most common reason beyond four years post-primary THA (after aseptic loosening); around the knee (TKA), periprosthetic distal femur fractures occur in 0.3–2.5% and proximal tibial fractures in 0.5–1.7%
- Risk factors: osteoporosis (most important patient factor); cementless press-fit femoral stems (higher intraoperative fracture risk from hoop stresses during impaction); revision arthroplasty (distorted anatomy, thinner cortices); osteolysis (weakens the periimplant bone); prior cortical perforation; rheumatoid arthritis; neurological disease (fall risk); notching (for distal femur fractures around TKA); female sex; advanced age
- Timing: intraoperative periprosthetic fractures (recognised or unrecognised at index surgery) vs postoperative fractures; most postoperative fractures result from low-energy falls (87% of cases in published series); spontaneous fractures without preceding trauma occur in the presence of severe osteolysis; early postoperative fractures (within weeks of surgery) in cementless stems indicate that the stem was never adequately integrated
Vancouver Classification — Periprosthetic Hip (Femoral) Fractures
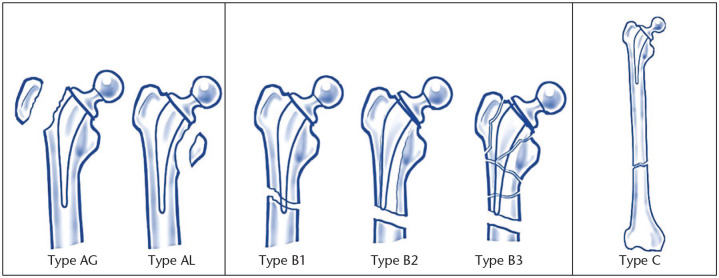
The Vancouver classification (Duncan and Masri, 1995) is the most widely used system for periprosthetic femoral fractures around a THA. It classifies fractures based on three parameters: fracture location relative to the stem, implant stability, and bone stock quality. It has been validated for reliability and reproducibility (kappa values 0.61–0.83 for inter- and intraobserver agreement).
| Vancouver Type | Location / Features | Implant Stability | Bone Stock | Management |
|---|---|---|---|---|
| Type AG | Greater trochanter avulsion | Stem stable | Good | Conservative if minimally displaced; ORIF with tension band wire or cables + plate if displaced (>2 cm) or abductor insufficiency |
| Type AL | Lesser trochanter | Stem stable | Good | Conservative in most cases; rarely requires fixation; may indicate calcar stress riser |
| Type B1 | Around stem or just below tip | Stem WELL FIXED | Good | ORIF — locking plate (pre-contoured periprosthetic plate with cable-plate system; locking screws above and below, cerclage cables around the stem); retain the well-fixed stem |
| Type B2 | Around stem or just below tip | Stem LOOSE | Good proximal bone | Revision arthroplasty with long cementless bypass stem (stem bypasses fracture by 2 cortical diameters distally); the fracture is then stabilised by the stem as it bridges it; cerclage cables may supplement; ORIF alone for B2 produces high failure rates — the loose stem must be addressed |
| Type B3 | Around stem or just below tip | Stem LOOSE | POOR proximal bone stock (severe osteoporosis, osteolysis, comminution) | Revision arthroplasty with long stem + structural allograft (strut allograft or impaction grafting); distal femoral replacement mega-prosthesis; proximal femoral replacement for very severe proximal bone loss; most complex category |
| Type C | Well below the stem tip (distal femur / femoral shaft) | Stem unrelated to fracture | Variable | Treat as an independent femoral fracture; ORIF with plate (avoiding the stem); IM nail if canal is clear distal to the stem tip; the implant is retained; standard trauma principles apply |
The B1 vs B2 Distinction — The Critical Decision
- The most important and most difficult pre-operative decision in Vancouver B fractures is distinguishing B1 (stable stem — ORIF) from B2 (loose stem — revision); getting this wrong has serious consequences: ORIF of a loose B2 stem fails reliably; studies show up to 47% of stems classified as stable pre-operatively are found to be loose intraoperatively — the `unknown loose stem` problem (Swedish Hip Registry data); pre-operative radiographic criteria suggesting loosening: progressive radiolucent lines >2 mm, component subsidence (compare with previous X-rays), cement mantle fracture, osteolysis, pedestal sign at the stem tip (cortical density at the tip = fibrous ingrowth, not osseointegration); clinical criteria suggesting loosening: pre-fracture thigh pain on weight-bearing (start-up pain), reduced mobility prior to the fracture event
- Intraoperative testing remains the gold standard: even after careful pre-operative assessment, definitive stem stability is only confirmed intraoperatively; when the fracture is exposed, the stem is tested for mobility (translation and rotation) relative to the proximal femoral fragment; a mobile stem = loose = revision required; equipment for both fixation (periprosthetic plates, cables) AND revision (long bypass stems, revision components) must be available at the time of surgery
- The B2 controversy — ORIF vs revision: the standard teaching is that B2 (loose stem) requires revision with a long bypass stem; however, a growing body of evidence supports ORIF with locking plates as a viable alternative in selected B2 fractures, particularly in frail, elderly, high-anaesthetic-risk patients where revision surgery carries prohibitive risk; relative indications for ORIF in B2 include Parker Mobility Score <5, ASA ≥3, high Charlson Comorbidity Index, and surgeon preference in low-functional-demand patients; relative indications for revision in B2 include good functional demand, younger age, and reconstructable bone stock
Periprosthetic Acetabular Fractures
- Less common than femoral periprosthetic fractures; 7–8 of 10 occur intraoperatively during cup reaming or press-fit impaction; classified by the Della Valle and Paprosky system or the Unified Classification System (UCS)
- Intraoperative acetabular fractures: recognised during surgery — if the cup is still stable and the fracture is non-displaced, conservative management (protected weight-bearing for 6–8 weeks) may suffice; if the cup is unstable or the fracture involves the posterior column (the main structural support) → cup removal, fracture fixation with plate ± screws, and cup reimplantation with augments or a cage if needed; these fractures can be missed intraoperatively — if the patient fails to mobilise post-operatively or develops pain disproportionate to the procedure, a post-operative CT should be obtained
Periprosthetic Fractures around TKA
- See dedicated articles for Lewis-Rorabeck (distal femur) and Felix (proximal tibia) classifications covered in the TKA periprosthetic fractures article; key principles: distinguish stable vs loose implant; ORIF (RIMN or DFLP) for stable implant; revision with long stemmed component for loose implant; RIMN requires open-box femoral component (CR TKA) — closed box PS TKA requires DFLP instead
- Anterior femoral notching and TKA fractures: a specific risk factor for supracondylar periprosthetic fractures around TKA — notching >3 mm reduces the fracture load of the distal femur by 18–30%; risk is 2–3× higher; anterior notch = stress riser; prevention by careful femoral sizing and intraoperative fluoroscopic confirmation of the anterior cut level
Surgical Fixation Principles
- Periprosthetic locking plates: pre-contoured anatomical plates designed specifically for periprosthetic femoral fractures (DePuy Synthes LISS, Stryker Peri-Loc, Zimmer Periarticular); key features — locking screws in the distal segment that can be directed to avoid the implant stem; cable/cerclage slots or holes to allow cables to wrap around the femoral cortex proximally (where screws cannot be placed alongside the stem); variable-angle locking holes allow multidirectional screw placement to find available bone around the stem; the plate acts as a bridging construct (relative stability — callus healing) not a compression plate
- Two-cortical-diameter bypass rule for revision stems: a long bypass stem used for B2/B3 revision must extend beyond the most distal fracture line by at least two femoral cortical diameters; this ensures the fracture is adequately bridged and the distal fixation zone is sufficient to prevent cantilever bending failure
- Strut allograft: cortical strut allografts (from the tibial or fibular shaft) are applied as biological plates alongside the femoral cortex and secured with cerclage cables; they provide structural support, stimulate periosteal healing, and add bone stock — particularly useful in B3 fractures with severely deficient proximal femoral cortex; over time the strut allograft incorporates and hypertrophies; this technique (strut allograft + long bypass stem) is a key option for the most complex periprosthetic fractures
- Extended trochanteric osteotomy (ETO): a controlled osteotomy of the posterior proximal femoral cortex that is deliberately created to allow removal of a well-fixed cementless stem during revision surgery; the ETO allows direct access to the stem for extraction; at closure it is reattached with cerclage cables; the ETO is a planned, controlled fracture — it is not a complication but a surgical technique; it is used when a well-fixed stem must be revised (e.g., malpositioned stem, head-neck taper corrosion, periprosthetic infection requiring component removal)
Exam Pearls
- Vancouver classification (THA): AG/AL (trochanteric); B1 (around stem, stable — ORIF); B2 (around stem, LOOSE, good bone — revision + long bypass stem); B3 (around stem, loose, POOR bone — revision + strut allograft/proximal femoral replacement); C (below stem — treat as standard femoral fracture)
- B1 vs B2 — most critical distinction: ORIF for B1; revision for B2; ORIF of a loose B2 fails reliably; up to 47% of stems classified stable pre-op are loose intraoperatively (Swedish registry); pre-op loosening signs — radiolucent lines >2 mm, subsidence on serial X-rays, pedestal sign, pre-fracture start-up thigh pain
- Two-cortical-diameter rule: bypass stem must extend beyond distal fracture line by ≥2 cortical diameters; shorter bridging = cantilever failure at the fracture
- Intraoperative acetabular fracture: usually during press-fit cup impaction; stable non-displaced — protected weight-bearing; unstable or posterior column involved — cup removal + posterior column plate + reimplant with augment/cage
- Intraoperative THA femoral fracture: cementless stems much higher risk (5.4%) vs cemented (0.3%); calcar crack → cerclage wire before/after stem impaction; more extensive → longer stem; always fluoroscope after impaction
- Periprosthetic locking plates: pre-contoured anatomical design; locking screws distal to stem (multidirectional); cerclage cables proximal (alongside stem); bridging construct principle; relative stability; callus healing
- Strut allograft: cortical strut + cerclage cables; biological plate; for B3 with deficient proximal cortex; incorporates and hypertrophies over time; combined with long bypass stem
- Extended trochanteric osteotomy (ETO): controlled planned osteotomy for removal of well-fixed cementless stem; posterior proximal femoral cortex; closed with cerclage cables; not a complication — a deliberate surgical technique for revision
- Exclude infection: 11.6% of periprosthetic fractures have concurrent PJI; WCC/ESR/CRP positive predictive values are poor (18–29%) — aspirate if clinical suspicion; do not miss PJI before undertaking fracture fixation or revision
- Mortality: 15–20% at 1 year in frail elderly patients with periprosthetic hip fractures; multidisciplinary orthogeriatric co-management essential; anaesthetic risk assessment guides surgical approach (ORIF vs revision for B2 in frail patients)